Trigeminal neuralgia(TN) is a disorder of the 5th cranial nerve that causes stabbing or electric shock like pain in parts of the face. This pain comes directly from the trigeminal nerve in the face and can affect all of the face and part of the eye. The trigeminal nerve is responsible for carrying pain, feelings and other sensations from the brain to the parts of the face. This condition does not specifically target any certain age or race and maybe be considered a normal part of the aging process. Trigeminal neuralgia most often occurs due to increased pressure on the trigeminal nerve from a blood vessel or tumor, but can also be caused by multiple sclerosis. The most common symptom is very painful or sharp electric feeling pain that lasts a few minutes but may become constant. Pain maybe triggered by light touch or stimulus and usually only occurs on one side of the face around the eye, cheek and lower part of the face. Often times the painful experience arises after trauma to the face or neck, such as whiplash.
To fully diagnose trigeminal neuralgia a variety of exams are performed such as a neurological exam. MRI is the typical imaging study used to diagnose trigeminal neuralgia. MRI will most often reveal a slow-growing brain tumor compressing the nerve. Treatment options do exist and have proven to be successful in reducing the amount of attacks and the severity of pain. Treatment options include anti-convulsive drugs or surgery.

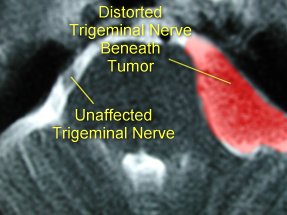
MRI axial image of the trigeminal nerve being compressed beneath a tumor causing TN compared to a normal trigeminal nerve.








